Here are
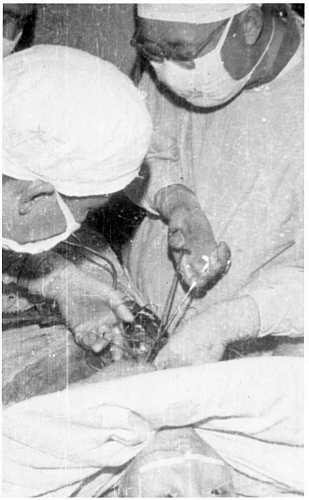
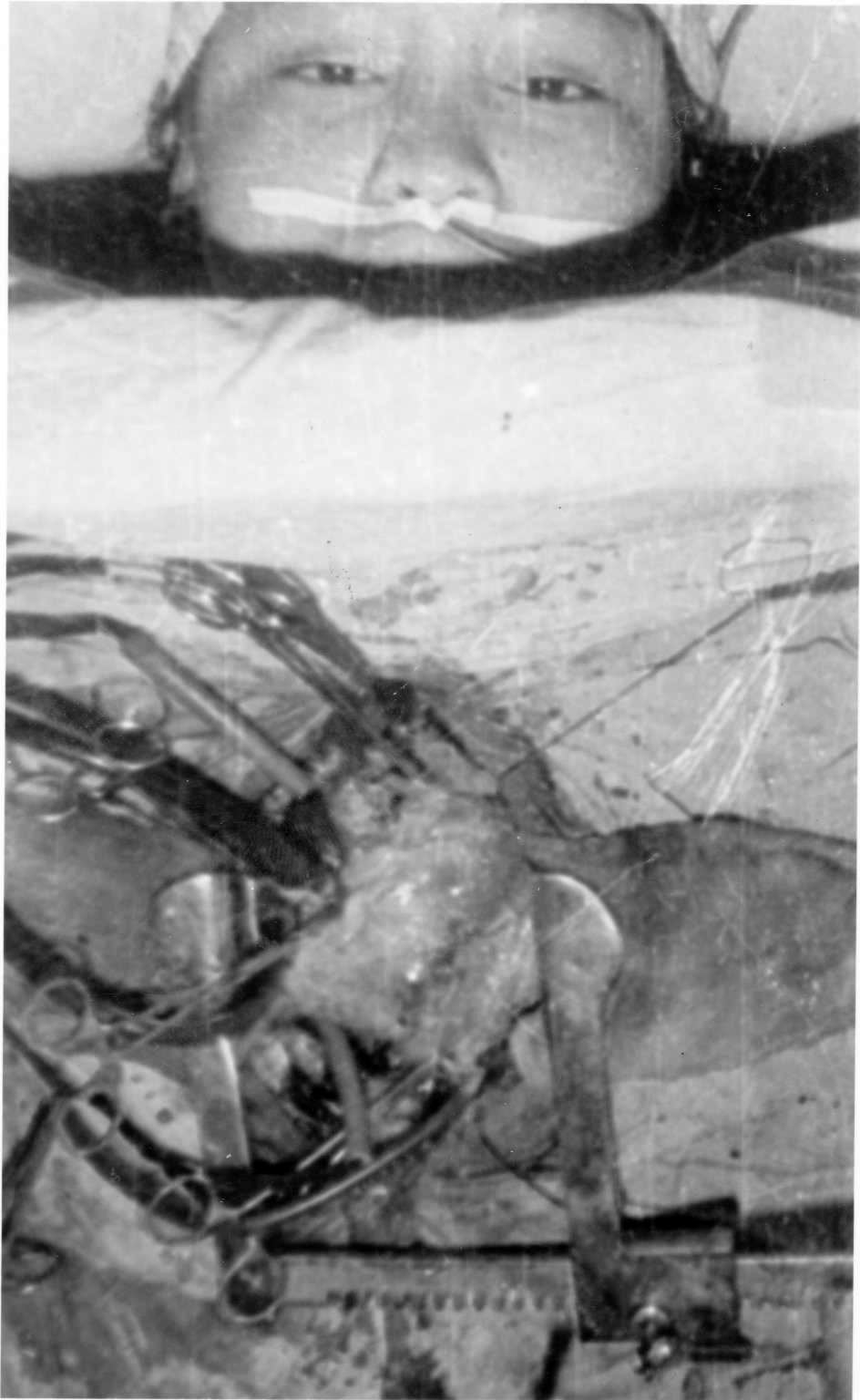
some pictures of open heart surgery with acupuncture anaesthesia with the patient
awake and talking, performed around 35 years ago in Hangzhou. In discussions
I had with the surgeon Dr Zhou, he said he needed to interview and choose canditates
dependant on their personality. He said while operating he needed to make slower
and more careful movements, to minimise discomfort. He also mentioned that the
recovery time was quicker and with less complications when compared to a general
anaesthetic. It was pictures like these that came out of China in the 70s
that stimulated much interest from the West and many early research visits to
China.
s
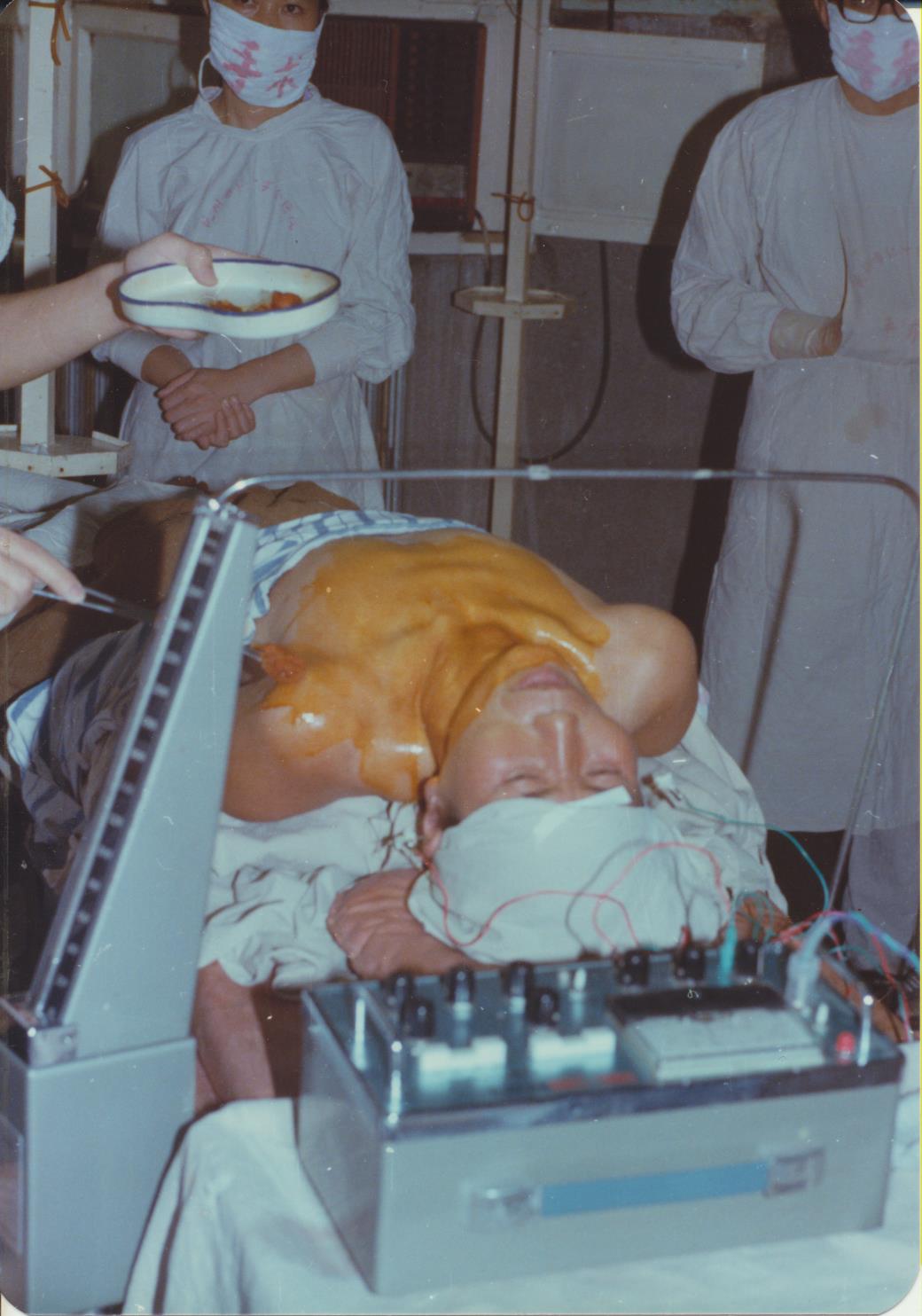
The following images were taken by myself in the Hanzhou 2nd Red cross
hospital in 1984. The operation was removal of 1/2 a thyroid under acupuncture
anaesthesia. During the operation the patient asked for a cup of tea. The answer
from the surgeons was that the tea would have to be delayed a while as they
were operating on the throat area. The electro-acupuncture stimulator can be
seen in the first image. Acupuncture with strong stimulation is used, combined
with strong electro-stimulation.
Research
Acupuncture anesthesia for open heart surgery in contemporary China.
Zhou J, Chi H, Cheng TO, Chen TY, Wu YY, Zhou WX, Shen WD, Yuan L. Abstract
BACKGROUND:
Although the use of acupuncture anesthesia for open heart surgery, which was introduced
in China four decades ago, has declined in recent years, there is a renewed interest
in it in contemporary China due to the escalating medical costs associated with
open heart surgery. This study was aimed to determine whether a combined acupuncture-medicine
anesthesia (CAMA) strategy reduces early postoperative morbidity and medical costs
in patients undergoing open heart operation under cardiopulmonary bypass.
METHODS:
From July 2006 to October 2010, CAMA was applied in 100 patients undergoing open
heart surgery in comparison with another 100 patients under the conventional general
anesthesia (GA). For all the CAMA patients, an abdominal breathing training program
was practiced for the 3 consecutive days prior to operation. About 15 to 20 min
prior to surgical incision, acupuncture needles were inserted into the bilateral
points ZhongFu, LieQue, and XiMen. During operation, patients were kept on spontaneous
breathing. Endotracheal intubation was not employed but only prepared as a standby.
The narcotic drugs, fentanyl and midazolam, were intravenously injected but in
very low doses as compared to GA. Open heart procedures were performed routinely
in both groups.
RESULTS:
Compared with the GA patients, the CAMA patients had a less usage of narcotic
drugs (p<0.001), less postoperative pulmonary infection (p<0.05), shorter
stay in intensive care unit (p<0.05), and a lower medical cost (P<0.05).
CONCLUSIONS:
A combined acupuncture-medicine anesthesia strategy reduces the postoperative
morbidity and medical costs in patients undergoing open heart surgery under cardiopulmonary
bypass.
PMID: 21570137 DOI: 10.1016/j.ijcard.2011.04.002 Int J Cardiol. 2011 Jul
1;150(1):12-6. doi: 10.1016/j.ijcard.2011.04.002. Epub 2011 May 12. ncbi.nlm.nih.gov



 s
s